Shoulder impingement syndrome is sometimes called swimmer’s shoulder, or thrower’s shoulder. It is caused by the tendons of the rotator cuff becoming trapped as they pass through the shoulder joint.
Impingement syndrome symptoms
Symptoms of impingement syndrome in the shoulder include:
- Shoulder pain with develops gradually over a period of days or weeks.
- Symptoms are worse during overhead movements such as in throwing, racket sports, and swimming.
- Pain may be located to the front and outside of your shoulder joint.
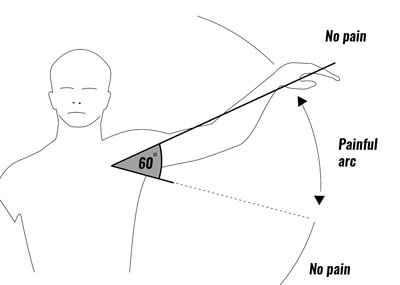
- In particular you will have pain over a 60 degree arc when lifting your arms out sideways and above your head.
- A professional therapist will perform a number of assessment tests to help diagnose your shoulder impingement including the ‘Empty can test’, ‘Neers test’ and ‘Hawkins-Kennedy test’.
- More on Impingement syndrome diagnosis
What is shoulder impingement syndrome?
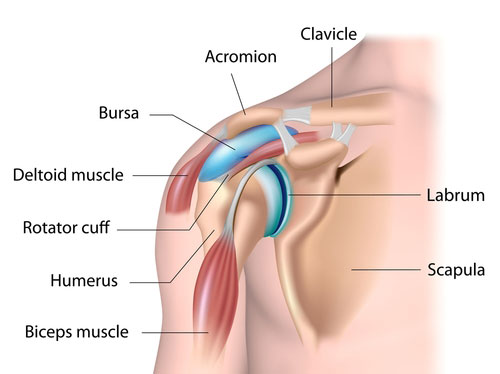
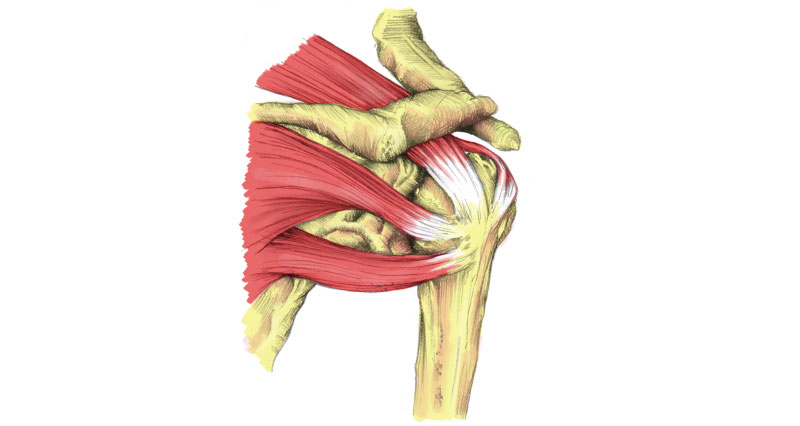
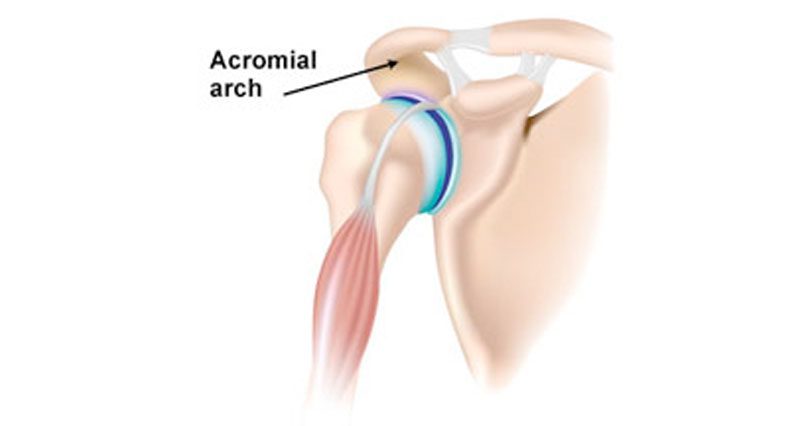
Impingement of the shoulder, which is sometimes called swimmer’s shoulder or thrower’s shoulder, is caused by the tendons of the rotator cuff muscles becoming trapped or impinged as they pass through a narrow bony channel. This channel is called the subacromial space and so-called because it is under the arch of the acromion.
With repetitive pinching, the tendons become irritated and inflamed. This can lead to thickening of the tendon which may cause further problems because there is even less free space.
This is a viscous circle where the tendons become larger, they are impinged further by the structures of the shoulder joint and the muscles themselves.
Types of shoulder impingement
Shoulder impingement is classified as internal or external depending on the causes:
Internal impingement
This occurs predominantly in athletes where throwing is the main part of the sport, e.g. pitches in baseball or javelin throwers. The underside of the rotator cuff tendons impinges against the glenoid labrum.
This tends to cause pain at the back of the shoulder joint as well as sometimes at the front.
External impingement
External shoulder impingement is classified as primary or secondary.
Primary external impingement – is usually due to bony abnormalities in the shape of the acromial arch in the shoulder joint.
It can sometimes be due to congenital abnormalities are known as os acromial, or due to degenerative changes, where small spurs of bone grow out from the arch with age, and impinge on the tendons.
Secondary external impingement – is usually due to poor scapular or shoulder blade stabilization which alters the physical position of the acromion, hence causing impingement on the tendons.
Is often due to a weak serratus anterior muscle and a tight pectoralis minor muscles. Other causes can include weakening of the rotator cuff tendons due to overuse for example in throwing and swimming, or muscular imbalance with the deltoid muscle and rotator cuff muscles.
What causes shoulder impingement?
Impingement Syndrome in itself is not a diagnosis, it is a clinical sign. There are at least nine different diagnoses which can cause impingement syndrome. These include:
- Bone spurs – this is ossification, or tiny pieces of bone growing which impinge on the tendons.
- Rotator cuff injury – a tear or strain on one of the rotator cuff tendons.
- Labral injury – a tear or damage to the labrum which lines the shoulder joint.
- Shoulder instability – occurs when the shoulder partially dislocates.
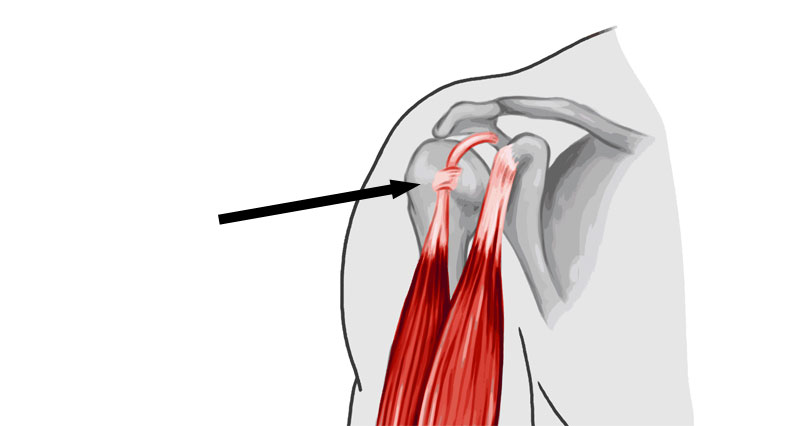
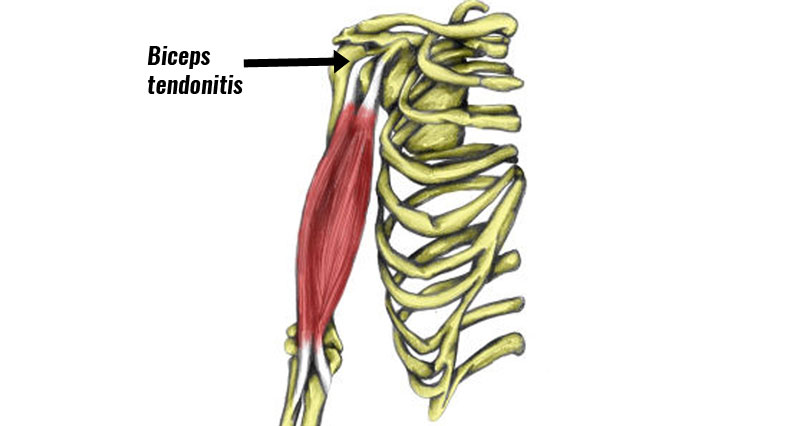
- Biceps tendinopathy – injury to the tendon of the biceps muscle.
- Scapula dysfunction – sbnormal movement pattens of the shoulder blade or shoulder girdle.
It is thought shoulder impingement begins as an overuse injury of the supraspinatus tendon which runs along the top of the shoulder blade.
Pain then prevents the rotator cuff muscles from working properly which causes the upper arm bone to shift slightly. This may also result in inflammation of the bursa or small sack of fluid (subacromial bursitis).
Over time the pain causes more dysfunction and impingement in a vicious circle which may eventually lead to ossification or bony spurs growing and causing injury to the rotator cuff tendons and so on.
If left untreated, shoulder impingement can develop into a rotator cuff tear. It is possible to have bony spurs growing but not have impingement symptoms.
Shoulder impingement syndrome treatment
The aim of a shoulder impingement syndrome rehab program is to reduce pain and inflammation, improve or maintain mobility of the shoulder, strengthen any weak muscles and correct postural problems before returning to full fitness.
Cold therapy/ice

Apply ice or cold therapy and compression wrap to the painful area for 10-15 minutes per hour initially reducing to 3 or 4 times a day as symptoms reduce.
Remember to use an ice bag or a towel wrapped around the ice to protect against ice burn.
Rest
This is particularly important. Rest the shoulder from any painful activities or movements. Pain indicates increased inflammation and delaying the healing process.
Maintain aerobic fitness on a stationary cycle. This period of rest, icing and anti-inflammatory medication should last up to a week.
Medication
NSAID’s (Non-Steroidal Anti-Inflammatory Drugs) e.g. Ibuprofen may be prescribed by a doctor. Athletes with asthma should not take Ibuprofen.
Medication may help in the early stages of rehabilitation (first few days), but longer-term it is though they are unlikely to help as much.
Electrotherapy
A professional therapist may also use electrotherapy such as ultrasound to reduce pain and inflammation. Ultrasound therapy transmits high frequency sound waves into the tissues for a micro massage effect.
- More on electrotherapy
Massage
Sports massage can be used to help relax any tight muscles, such as the rotator cuff and upper back muscles. Cross friction massage techqniques may be applied to the shoulder tendons.
- More on Sports massage
Corticosteroid injection
They may discuss the option of directly injected steroids into the subacromial space to reduce inflammation and reduce inflammation in the local area although this is not usually an early option. It is usually recommended after a period of at least 6-12 months.
Correct postural issues
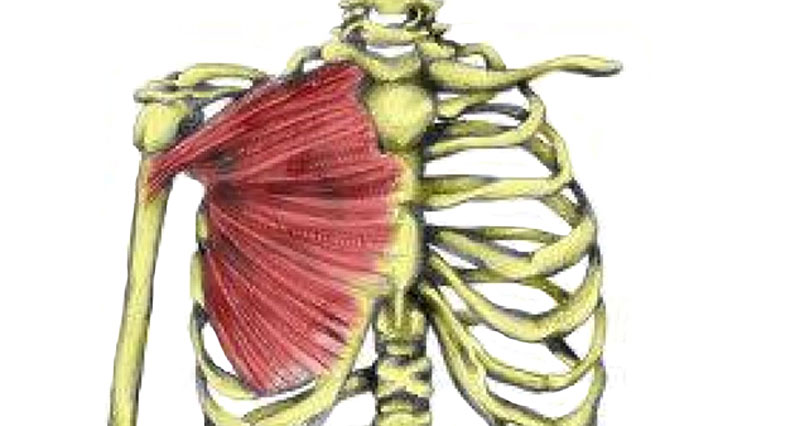
Shoulder impingements are common in individuals with poor posture and scapula (shoulder blade) movement dysfunctions. This is often caused by tightnesses in the chest muscles (especially pectoralis minor), which pull the scapula forward.
Also, weakness in the upper back muscles, particularly serratus anterior, which allows the shoulder blade to be pulled forward by the chest muscles.
Working on improving the posture can begin from day one, through demonstrations of good posture and chest stretching. This can be progressed to include scapula setting and stabilisation exercises.
Exercises

Both mobility and strengthening exercises are important. Mobility exercises should begin as soon as pain will allow and should avoid any areas of movement that do cause pain.
As your symptoms improve, strengthening exercises can begin but within the limits of pain. In particular, rotator cuff strengthening and shoulder stability exercises are important.
- More on shoulder impingement exercises
References & further reading
- Seitz AL, McClure PW, Finucane S et al. Mechanisms of rotator cuff tendinopathy: intrinsic, extrinsic, or both? Clin Biomech (Bristol, Avon) 2011;26(1):1–12
- Wilk KE, Obma P, Simpson CD et al. Shoulder injuries in the overhead athlete. J Orthop Sports Phys Ther 2009;39(2):38–54.
- Balke M, Schmidt C, Dedy N et al. Correlation of acromial morphology with impingement syndrome and rotator cuff tears. Acta Orthop 2013;84(2):178–83.