Shoulder pain is either acute (sudden onset) or chronic (gradual onset) caused by overuse. Long term shoulder pain is often related to overuse.
Select the type or location of your shoulder pain:
Acute shoulder pain
Sudden onset or acute shoulder injuries often occur following a fall onto an outstretched arm, from a direct impact or trauma, overstretching or overloading the joint.
Rotator cuff strain

A rotator cuff strain is a common cause of acute shoulder pain in sports, especially in throwing and racket sports. It is a tear to any of the four ‘rotator cuff’ muscles in the shoulder. Symptoms include:
- Sudden shoulder pain which may radiate down into the arm.
- You may have a feeling that something has torn.
- Rotator cuff strains can be mild or very severe.
- Read more on rotator cuff strain
Acromioclavicular joint sprain
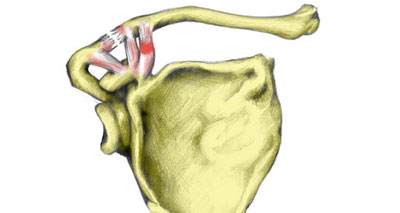
An AC joint separation or AC joint sprain is a tear to the ligament that joins the acromion and clavicular bones at the top of the shoulder. It is often caused by falling onto an outstretched arm. Symptoms include:
- Severe pain which often radiates throughout the shoulder joint.
- A lump or swelling on the bony bit on the top of your shoulder.
- Widespread pain throughout the shoulder immediately after injury
- Later pain is localized to the top of the shoulder
- Symptoms are worse when moving the arm out sideways and overhead.
- A lump on top of the shoulder or deformity is visible in severe cases.
- More on ac joint separation.
Dislocated shoulder
A dislocated shoulder is a very traumatic and painful injury. It occurs when the head of the humerus (upper arm bone) pops out of the shoulder joint. Symptoms include:
- Sudden, severe pain at the time of injury.
- Your shoulder joint will swell up rapidly.
- You will be unable to move your arm.
It is essential you seek medical attention immediately. DO NOT attempt to pop your shoulder back in because this can cause permanent injury to nerves and blood vessels.
- More on a dislocated shoulder
Long head of biceps rupture

A rupture of the long head of biceps muscle is a tear or strain of the long tendon of the biceps muscle which originates from the shoulder. It is more common in older athletes.
- Sudden sharp pain is felt at the front of the upper arm/shoulder.
- There may be pain and swelling over the front of the shoulder joint.
- Contracting the biceps muscle against resistance is likely to be painful.
- In particular, lifting a straight arm up forwards against resistance will reproduce symptoms.
- More on the rupture of the long head of biceps
Broken collar bone (Clavicle fracture)
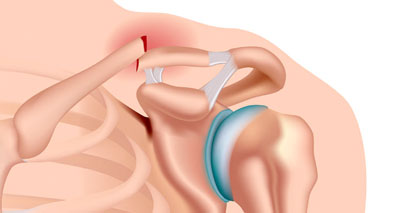
A Clavicle fracture is also known as a broken collarbone. You can fracture your collarbone by falling onto an outstretched arm or your shoulder.
- You will feel severe pain in the collarbone with swelling.
- If you suspect you have a broken collar bone seek medical attention immediately.
- More on clavicle fracture
Pec major tendon strain
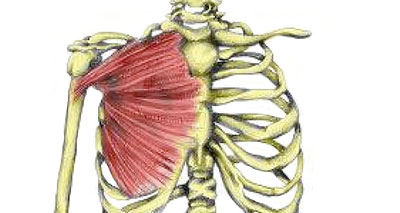
A pectoralis major tendon strain is a strain or tear of the powerful pectoralis major muscle at the front of the chest. The pectoralis muscle rotates the arm inwards and is at its weakest where it attaches to the humerus (arm) bone. Symptoms include shoulder pain and swelling at the front of the shoulder.
- More on pectoralis major tendon strain
- View all acute shoulder injuries
Chronic shoulder pain
Gradual onset shoulder pain or chronic shoulder pain develops over a period of time. You may not have known the exact time of injury and put up with a ‘niggle’, or discomfort for some time.
Rotator cuff tendinopathy (tendonitis)
Rotator cuff tendinopathy is a degenerative condition affecting one or more of the rotator cuff tendons in the shoulder.
- Pain is often present when resting.
- It is made worse by lifting things, especially above your shoulder.
- The tendon will probably feel tender and there may be a creaking feeling when the shoulder moves.
- More on rotator cuff tendinopathy
Shoulder impingement syndrome
Impingement of the shoulder, sometimes called swimmer’s shoulder or thrower’s shoulder, is caused by the tendons of the rotator cuff muscles becoming trapped or impinged. Symptoms include:
- Shoulder pain develops gradually over a period of days or weeks.
- Pain may be located to the front and/or outside of your shoulder joint.
- Symptoms are worse during overhead movements such as in throwing, racket sports, and swimming.
- More on shoulder impingement
Frozen shoulder

A frozen shoulder causes pain and restricted movement in the shoulder joint. It is normally only seen in older people, with no specific cause. There are three phases to this injury.
- Initially, the shoulder will ache, with the pain becoming more widespread and worse at night.
- The joint will then start to stiffen and the pain may limit daily activities.
- Eventually, with treatment, your shoulder will begin to loosen up and the pain will ease.
- More on frozen shoulder
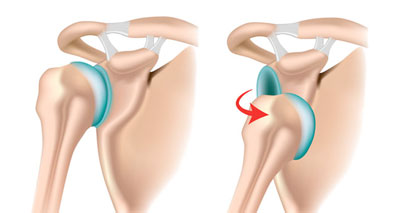
Glenoid labrum tear
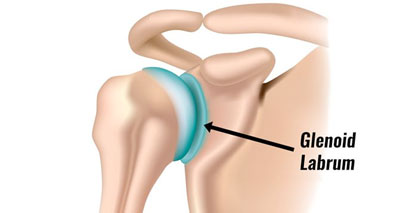
Glenoid labrum tear occurs when the tissue lining the shoulder joint socket tears. It is more common in sports which involve repetitive movements such as overhead throwing.
Symptoms include:
- Weakness and pain in your shoulder joint.
- Resisted flexion (bending) of the elbow and moving the arm behind your back may reproduce symptoms.
- More on glenoid labrum tear
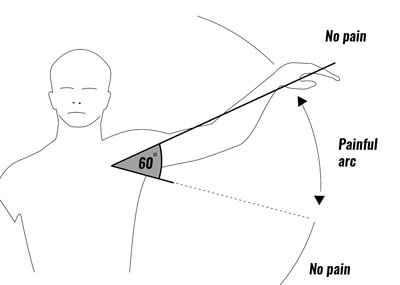
Subacromial bursitis

Subacromial bursitis has similar symptoms to Supraspinatus tendinitis. A bursa is a small sack of fluid found between the tendon and bone. The bursa can become impinged or trapped in the shoulder.
- This results in pain and weakness in the arm, particularly when it is lifted sideways through a 60-degree arc.
- Pain may also be felt when you press in at the inside front of the upper arm.
- More on subacromial bursitis
Winged scapula
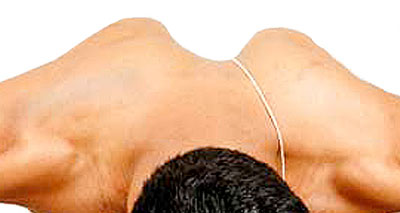
A winged scapula is a symptom of another condition, rather than an injury itself.
- It is where the shoulder blade protrudes out on the back, rather than lying flat against the back of the chest wall.
- A winged scapula can be painful.
- It may be linked to poor posture, which is quite common with many people sitting at desks all-day
- More on the winged scapula
Suprascapular Neuropathy
Suprascapular neuropathy usually occurs as a result of traction damage to the suprascapular nerve, causing an aching or burning pain at the back and or side of the shoulder joint.
- Aching or burning pain will be felt at the back and or side of the shoulder joint.
- The pain will come on gradually and feel like it is deep within the shoulder joint and may radiate through the arm.
- Weakness of the shoulder joint will be experienced by the patient when lifting the arm out to the side and rotating it outwards.
- Over time there may be a visible wasting of the supraspinatus and infraspinatus muscles.
- More on suprascapular neuropathy
Shoulder rehabilitation & exercises
- Rotator cuff exercises
- AC joint sprain rehabilitation
- Dislocated shoulder rehabilitation
- Shoulder stability exercises
- Functional shoulder exercises
- General shoulder rehabilitation exercises
References & further reading
- Seitz AL, McClure PW, Finucane S et al. Mechanisms of rotator cuff tendinopathy: intrinsic, extrinsic, or both? Clin Biomech (Bristol, Avon) 2011;26(1):1–12
- Wilk KE, Obma P, Simpson CD et al. Shoulder injuries in the overhead athlete. J Orthop Sports Phys Ther 2009;39(2):38–54.