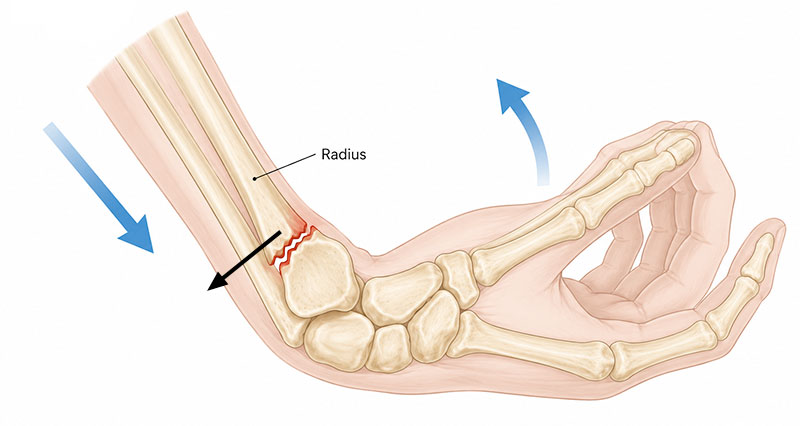
A Rolando fracture is a severe fracture at the base of the thumb where the thumb metacarpal joins the wrist. It is similar to a Bennett fracture, but more complex because the bone breaks into multiple fragments. Rolando fractures commonly occur following a punch to a hard object, a fall, or direct trauma during contact sports or road traffic accidents. These fractures are usually unstable and almost always require surgery.
On this page:
ADVERT
Symptoms of a Rolando fracture
Symptoms usually develop immediately after injury and may include:
- Severe pain at the base of the thumb
- Rapid swelling around the thumb and wrist
- Bruising which develops over the following hours
- Difficulty or inability to grip objects
- Severe pain moving the thumb
- Tenderness directly over the base of the thumb
- Visible deformity if the fracture fragments are displaced
Diagnosis
A doctor or physiotherapist will examine the thumb and hand for swelling, deformity and tenderness. X-rays are normally required to confirm the diagnosis and assess how many fracture fragments are present. In more complex injuries, a CT scan may be used to assess the fracture in greater detail before surgery.
What is a Rolando fracture?
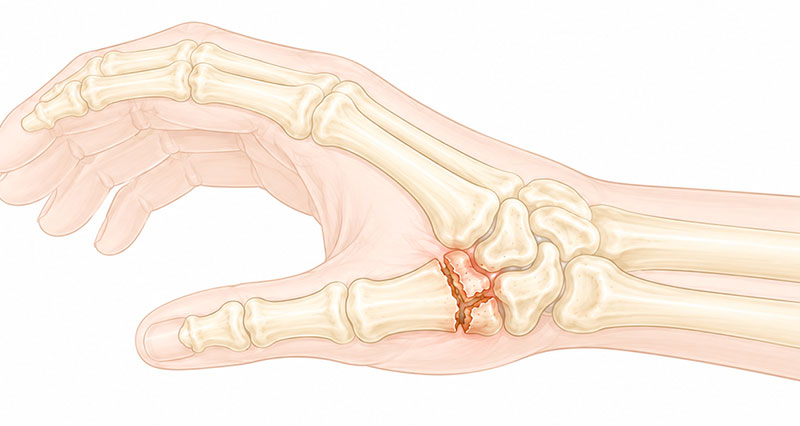
A Rolando fracture affects the carpometacarpal (CMC) joint of the thumb. This is the joint where the first metacarpal bone meets the trapezium bone in the wrist.
Unlike a Bennett fracture, where there is usually a single fracture line, a Rolando fracture involves multiple fracture fragments. The break often forms a characteristic T-shaped or Y-shaped pattern.
The thumb CMC joint is extremely important for grip strength, pinching and hand function. Because the fracture extends into the joint surface, accurate treatment is essential to reduce the risk of long-term stiffness, weakness and arthritis.
Causes
Common causes include:
- Punching a hard object
- Falling onto the thumb or hand
- Sporting injuries
- Road traffic accidents
- Direct impact injuries
These fractures are more common in contact sports and activities involving falls or high-impact trauma.
Treatment for a Rolando fracture
Surgery is almost always required. It is essential that all the bone fragments are put back in place and pinned, or screwed if needed. The procedure involves realigning the bone fragments and then fixing them with internal wires or pins.
In some cases, an external frame with pins is used. The joint is then immobilized for 4 to 6 weeks in a thumb spica cast, where the thumb is kept separate from the hand. When the cast is removed, the patient is referred to a physiotherapist or physical therapist or similar who will help mobilize the joint.
Surgery
Mr Elliot Sorene MBBS FRCS (Tr & Orth) EDHS Consultant Orthopaedic, Hand & Upper Limb Surgeon explains about surgery for Rolando and Bennett’s Fractures.
Complications
Possible complications include:
- Stiffness in the thumb joint
- Reduced grip strength
- Ongoing pain
- Post-traumatic arthritis
- Weak pinch grip
- Poor fracture healing
- Loss of thumb mobility
Early treatment and a structured rehabilitation program help reduce the risk of long-term problems.
Rehabilitation exercises
Once the fracture has healed sufficiently, rehabilitation aims to restore movement, strength and hand function.
Rehabilitation may include:
- Gentle mobility exercises
- Thumb range of motion exercises
- Grip strengthening exercises
- Pinch grip exercises
- Hand and wrist strengthening
- Functional rehabilitation for sport or work activities
Recovery time & returning to sport
Recovery can take several months depending on the severity of the fracture and the type of surgery performed. Return to sport depends on the severity of the injury and the type of activity involved. Contact sports and activities involving gripping usually require a longer recovery period. A protective thumb splint or support may be recommended when returning to training or competition.
Recommended products for Smith’s fracture recovery
We recommend the following products from our commercial partners (Amazon) for helping with recovery from a Scaphoid fracture:
- Cold therapy wrap: Helps reduce pain, swelling and inflammation during the first few days after injury or surgery. Most appropriate during the acute phase and after rehabilitation exercises if swelling develops.
- Arm sling: Supports and protects the injured wrist whilst waiting for medical treatment or during the early stages of recovery. Helps reduce strain on the fracture site.
- Wrist support: Provides stability, reduces pain and helps confidence when coming out of the cast. Use for 1–3 weeks, then gradually reduce.
- Compression wrist support: Helps reduce mild swelling and improve comfort during later-stage recovery. Best used once healing has progressed and movement exercises have started.
- Therapy putty or hand exerciser: Rebuilds grip strength and targets muscles weakened during immobilisation. One of the most effective rehab tools.
- Hand exerciser/grip strengthener: Allows progressive resistance training and helps with return to sport-specific activity.
- Resistance bands: Used for wrist flexion, extension and radial deviation to restore full strength, not just grip.
- Cold therapy pack & Gel: Useful in the early rehab phase to reduce pain and control inflammation after exercise.
- Heat therapy: Helps reduce stiffness once swelling has settled and is useful before mobility exercises.