Shoulder subluxation, also known as shoulder instability, occurs when the shoulder joint partially dislocates. By its nature, the shoulder has a large range of movement making it naturally less stable than other joints.
What is shoulder subluxation?
No single structure is responsible for providing stability at the shoulder joint. The bones, ligaments, joint capsules, and muscles are all key components. They maintain a stable shoulder joint, yet permit a large range of movement in several directions.
Shoulder instability is often associated with subluxation or partial dislocation of the shoulder joint.
This is often what prompts the athlete to seek medical attention. In some people, a partial dislocation of the shoulder is not actually painful. It is more annoying, preventing them from taking part in daily activities or sports.
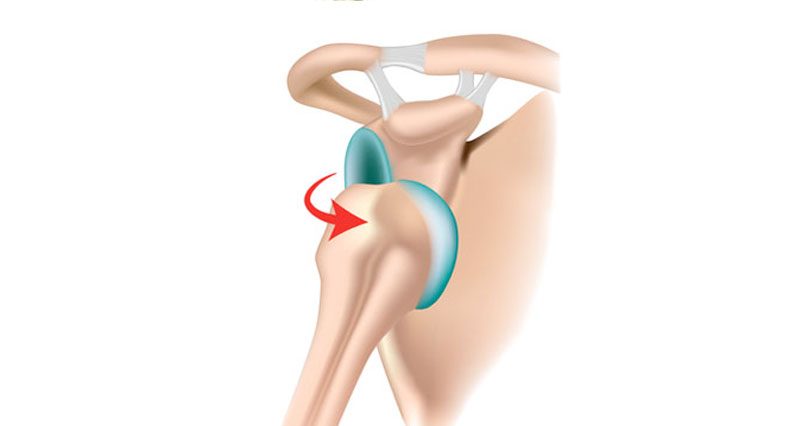
Shoulder subluxation can occur in one direction, for example, anterior instability where the arm or humerus bone pops out the front. Or posterior instability where it partially dislocates out the back or in more than one direction which is known as multi-directional instability. The most common form of instability seems to be anterior and is probably because the joint capsule is at its weakest at the front of the joint.
Causes
There are several reasons why the shoulder joint may be unstable and dislocated which are described below. Medical help from a physiotherapist will help as they can give exercises to help strengthen and stabilize the area.
There are many reasons why a shoulder may become unstable. If the joint surfaces are shaped slightly differently – for example, if the glenoid fossa is slightly flatter than usual, or the head of the humerus is more of an oval shape – the joint may not be as stable compared with other people who have “normal” joint anatomy.

Other structures support the bony anatomy to help provide stability to the shoulder. These include:
- Glenoid Labrum – a ring of cartilage which deepens the glenoid fossa, making the “cup” of the socket deeper and hence improving stability.
- Joint Capsule – a membrane which encompasses the entire joint, providing stability but also maintaining the joint complex and holding the lubricating (synovial) fluid in the correct place.
- Ligaments – holding the bones together and providing stability by preventing them from moving when they shouldn’t be.
- Muscles – Work alongside the ligaments in preventing unwanted movement, but also initiate and create a movement of the joint.
Shoulder instability may be caused by:
- Trauma (traumatic instability) Is usually due to a particular accident or injury which damages the structures that provide stability
- Sometimes an old injury – for example, an injury which weakens the capsule may cause instability – known as ‘post-traumatic instability’
- Joint Laxity (atraumatic instability) Maybe due to anatomical abnormalities generalised laxity (known as hypermobility) muscle weakness in certain conditions, including pregnancy
- Acute on chronic instability – a traumatic injury to an already lax joint
Treatment of shoulder subluxation
The therapist will perform a range of tests to determine what type of shoulder instability the athlete is experiencing, and will take a detailed history to attempt to discover why this is occurring. They will also assess whether you have a condition which has caused you to have lax ligaments throughout your body, known as Hypermobility.
A strengthening program to help you develop the muscles around the shoulder which are responsible for stabilizing the joint is usually recommended. A type of electrotherapy, similar to a TENS machine can allow the athlete to identify the muscles which are not working properly. A tiny electric current to make the muscle tingle helps the athlete to train the muscles more efficiently.
In some cases of instability (particularly traumatic instability), if conservative treatment with physiotherapy does not work, surgery may be an option. There are various techniques available to the surgeon to improve the joint laxity at the shoulder, however, this will always be followed by intensive rehabilitation to ensure that you do not lose any movement at the joint.
Arthroscopies are being used more frequently to diagnose the cause of instability. This is a minimally invasive procedure where you are given an anaesthetic, and a small fibre optic camera is introduced to the joint to inspect the structures and assess for any damage which might be repairable by surgery.