Groin Strain
A groin strain (pulled groin) is a tear of one or more adductor muscles on the inside of the thigh. Groin strains commonly occur during sprinting, twisting, kicking and rapid changes of direction in sports such as football, rugby and hockey. Symptoms range from mild tightness to severe pain and difficulty walking. Early treatment and a structured rehabilitation program are important to speed recovery and reduce the risk of recurrence.
Medically reviewed by Dr Chaminda Goonetilleke, 7th Jan. 2022
What are the symptoms of a groin strain?
- Sudden pain in the groin.
- Stretching your adductor (groin) muscles is painful.
- Pain squeezing your legs together.
- Swelling and bruising may develop but not always.
What does a pulled groin feel like?
Groin strains occur either in the belly of the muscle, or higher up where the tendon attaches to the pelvis. You will most likely feel a sudden sharp pain in the groin whilst running, twisting or turning. Symptoms range from mild discomfort to severe pain depending on how bad your injury is.
As a result, you may or may not be able to continue playing or training. Contracting your groin muscles (adduction) against resistance may be painful. For example squeezing your legs together with a ball between them reproduces symptoms.
How bad is my groin strain?
Groin strains are graded 1 to 3 depending on severity. Your doctor or physio performs a number of assessment tests to help diagnose groin pain.
Grade 1
A Grade 1 strain is a minor tear where less than 25% of fibers are damaged. You will have discomfort in the groin area, but should be able to walk with little or no pain.
Grade 2
A Grade 2 injury is a moderate tear involving damage to more than 25% of fibres. You feel a sudden sharp pain during exercise and may develop swelling and/or bruising.
Grade 3
Grade 3 groin strains are more serious involving a complete (100%) or almost complete rupture of the muscle. You will feel severe pain at the time of injury and be unable to walk properly. We recommend seeking professional medical attention as soon as possible.
- Learn more on how to diagnoise groin strains
Treatment for groin muscle strains
Treatment consists of immediate first aid followed by a full groin strain rehabilitation program.
If you think you have a pulled groin muscle then stop exercising immediately and apply the PRICE principles of protection, rest, ice, compression, and elevation.
Cold therapy
Apply a cold therapy and compression wrap for 10 to 15 minutes as soon as possible after injury. Repeat every 2 hours reducing frequency as your symptoms improve. However, continue for the first 48 hours, especially if it is a grade 2 or 3 injury.
This helps stop internal bleeding, reduces pain and swelling, speeding up the healing process. Do not apply ice directly to the skin because it may cause ice burns.

Groin strain strapping/taping

Protect your injured muscle by applying compression. Strap your leg with elastic bandage or wear a groin support. Compression helps stop bleeding and swelling as well as helping prevent further muscle damage.
Later in the rehabilitation process as you return to exercise, groin supports and compression shorts aid recovery by supporting your muscles, retaining heat and encouraging blood flow through the muscles.
Electrotherapy
Electrotherapy modalities such as ultrasound may be used to aid the healing process. Ultrasound transmits high-frequency waves into the tissues providing a micro-massage effect. It may also help disperse swelling.
Medication
Your doctor may prescribe NSAID medication such as Ibuprofen. NSAIDs are thought to be more beneficial in the early acute stages but less effective later on. Do not take Ibuprofen if you have asthma.
Groin strain massage
Sports massage is beneficial once the acute stage has passed. This is usually after 72 hours. Massage releases tension in the muscle and encourages blood flow. As a result, your muscle gets the nutrients needed for recovery.
However, be careful not to use massage too early because you may increase internal bleeding making your injury worse.
Exercises for pulled groin muscles
Our full Groin strain rehabilitation program is created by Professional Football Physiotherapist Paul Tanner. It is based on what Paul does with his elite players but adapted for use by anyone. It takes you step-by-step from injury to full fitness. Exercises should always be pain-free.
Stretching
It is important not to stretch your groin muscles too early, especially in the acute phase. Let them heal first! Once the acute phase has passed, begin gentle dynamic groin stretching exercises.
Strengthening
Similarly avoid specific groin strengthening in the early acute stages. When pain allows, begin isometric groin exercises. These involve contracting the muscles against resistance but without movement. Later, these are progressed to isotonic strengthening exercises which involve movement.
In addition we include:
- Activation exercises to keep your hip muscles firing and in good condition.
- Function exercises which are more sports specific and include plyometric exercises (hopping and bounding).
- Movement control exercises maintain and improve proprioception and balance.
- Condition exercises so you can maintain fitness.
Anatomy
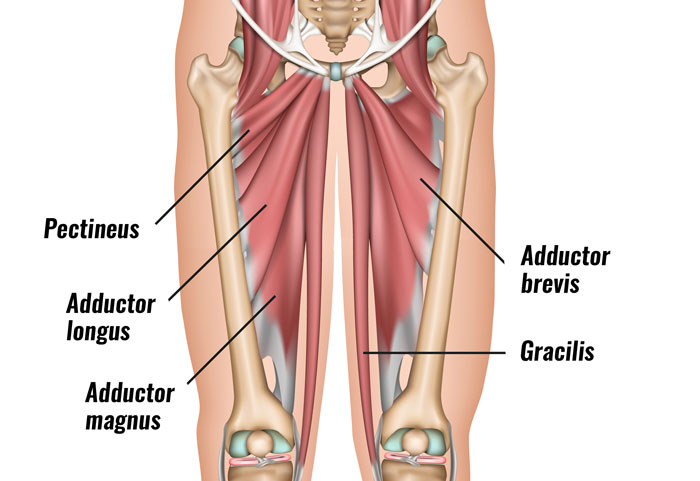
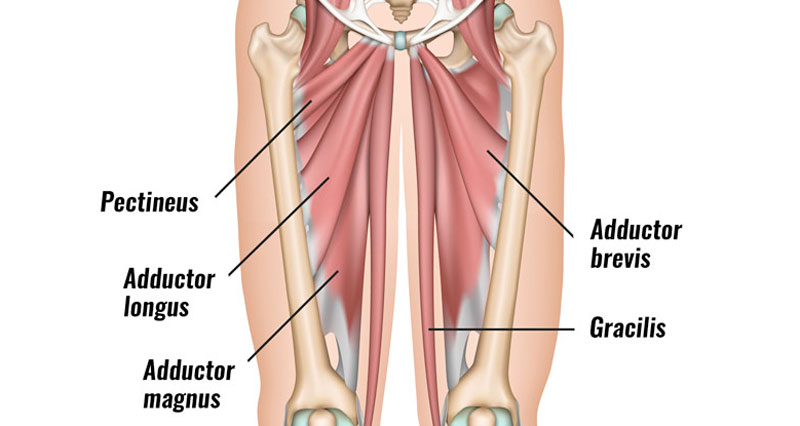
There are five groin (adductor) muscles, three short (pectineus, adductor brevis, and adductor longus) and two longer muscles (gracilis and adductor magnus). The short adductor muscles and adductor magnus attach above the knee. The gracilis inserts insert below the knee.
The main function of the adductor muscle group is to pull the leg inwards towards the midline (adduction). They also stabilize and control your pelvis during walking and running. Therefore they are especially important in any sport which requires rapid changes in direction.
How do I prevent Groin strains?
Although groin muscle strains can occur randomly there things you can do to mitigate the risk.
- Warm up properly.
- Strengtheing weak adductor muscles.
- Stretch regularly especially if you have tight adductor muscles.
- Make sure you have fully recovered from a previous groin injury.
- Be aware that lower back injuries/dysfunction as well as lower leg biomechanics can increase injury risk.
Groin strains usually occur when sprinting or changing direction quickly. Or from during rapid movements of the leg against resistance such as kicking a ball.
Overstretching the muscle such as in martial arts high kicks also causes torn adductors. It is also likely you may have damaged more than one structure if you experience a sudden onset of acute groin pain(1).
Injuries with similar symptoms
Other injuries which have similar groin pain symptoms include Gilmore’s groin and Adductor tendonitis.
References & further reading
- Serner A, Tol JL, Jomaah N, et al. Diagnosis of acute groin injuries: a prospective study of 110 athletes. Am J Sports Med 2015;43(8):1857–64.
- Serner A, van Eijck CH, Beumer BR, et al. Study quality on groin injury management remains low: a systematic review on the treatment of groin pain in athletes. Br J Sports Med 2015;49(12):813.
- Weir A, Brukner P, Delahunt E, et al. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br J Sports Med 2015;49:768–74.
- Hölmich P, Uhrskou P, Ulnits L et, al. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: a randomised trial. Lancet 1999;353:439–43.
Groin strain FAQ’s
A groin strain or pulled groin is a tear of an adductor muscle on the inside of the thigh. It occurs either within the belly of the muscle, or at the tendon where it attaches to the pelvis.
This depends on how bad your injury is but ranges from 1 week for mild strains to up to 8 weeks or more. Immediate first aid followed by rehabilitation exercises are important to prevent your injury recurring.
Most feel like a sudden sharp pain in the groin. Symptom range from tightness in your groin to severe pain. Squeezing your legs together often increases pain.


