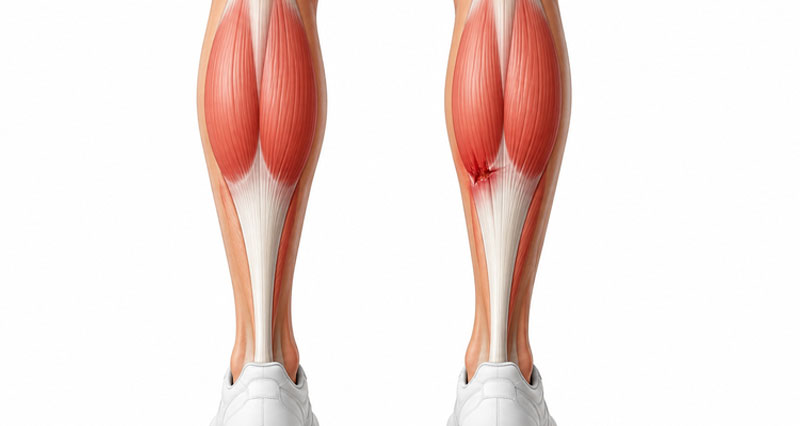
Posterior compartment syndrome occurs when pressure builds up within one of the muscle compartments of the lower leg. Increased pressure reduces blood flow and can affect muscles and nerves, causing pain, weakness and, in severe cases, permanent tissue damage. It may develop suddenly following an injury (acute compartment syndrome) or gradually during exercise (chronic exertional compartment syndrome).
On this page:
Important: Seek urgent medical attention immediately if you have severe calf or shin pain that is worsening, especially after an injury, fracture or direct blow. Acute compartment syndrome can cause permanent muscle and nerve damage if not treated promptly.
ADVERT


Symptoms of posterior compartment syndrome
Symptoms vary depending on whether the condition is acute (sudden onset) or chronic (exercise-induced).
Acute posterior compartment syndrome
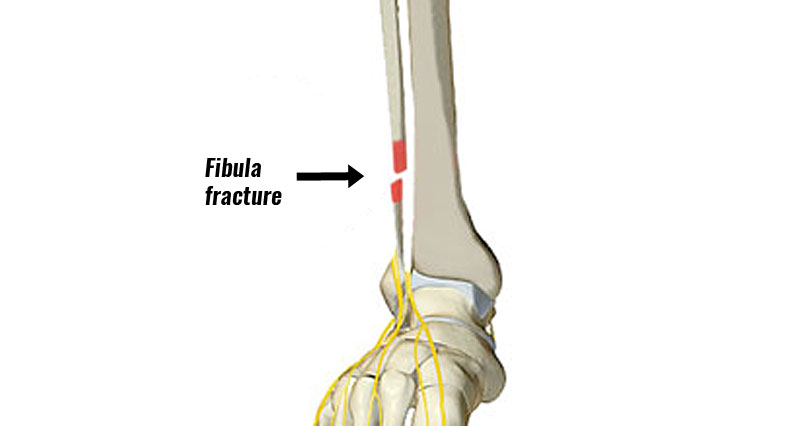
Acute compartment syndrome is a medical emergency and usually develops following a direct impact, fracture, crush injury, or severe muscle strain.
Symptoms may include:
- Severe pain in the calf or along the inside of the shin.
- Pain that becomes progressively worse over time.
- Pain that is out of proportion to the injury.
- Tightness or a feeling of pressure in the lower leg.
- Increased pain when moving the ankle or toes.
- Numbness, tingling, or altered sensation in the foot.
- Weakness of the foot and ankle in more severe cases.
Seek urgent medical attention immediately if you suspect acute compartment syndrome.
Chronic posterior compartment syndrome
Chronic exertional compartment syndrome develops gradually and is most common in runners and other endurance athletes.
Symptoms typically include:
- Deep aching pain along the inside of the shin or in the calf.
- Symptoms that begin at a predictable point during exercise.
- Pain that eases with rest but returns when activity resumes.
- A feeling of tightness, fullness, or pressure in the lower leg.
- Pain when pushing the foot downwards, such as when rising onto the toes.
- Numbness or pins and needles in the sole of the foot.
- Weakness or heaviness in the lower leg during exercise.
Some people may notice small lumps or bulges along the inside of the shin where muscle tissue protrudes through the surrounding fascia.
ADVERT


Diagnosis and compartment pressure testing
Deep posterior compartment syndrome can be difficult to diagnose because its symptoms are similar to other causes of shin and calf pain, including shin splints, stress fractures and tendon injuries.
Your doctor or physiotherapist will begin by taking a detailed history and examining your lower leg. They will want to know when symptoms occur, how quickly they come on during exercise, and how long they take to settle afterwards.
If they suspect chronic exertional compartment syndrome, they may perform compartment pressure tests. This involves inserting a small needle connected to a pressure monitor into the affected muscle compartment to measure the pressure within it.
Pressure measurements are usually taken at rest and repeated immediately after exercise. It is important that the exercise reproduces your symptoms, otherwise the test may not be accurate.
Raised compartment pressures, together with a typical history and examination findings, help confirm the diagnosis. Additionally, in some cases, using imaging such as MRI scans before and after exercise also supports the diagnosis.
Because deep posterior compartment syndrome often occurs alongside other lower leg conditions, it is important to rule out alternative causes of pain, including shin splints (medial tibial stress syndrome), tibial stress fractures, popliteal artery entrapment syndrome and peripheral artery disease.
ADVERT


What else could it be?
Deep posterior compartment syndrome may be mistaken for:
- Shin splints (medial tibial stress syndrome)
- Tibial stress fracture
- Tibialis posterior tendinopathy
- Calf muscle strain
- Popliteal artery entrapment syndrome
- Peripheral artery disease (vascular claudication)
- Nerve entrapment syndromes
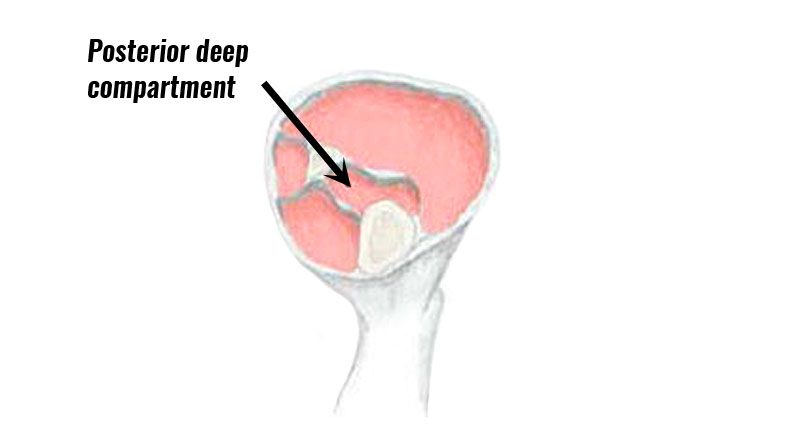
What is posterior compartment syndrome?
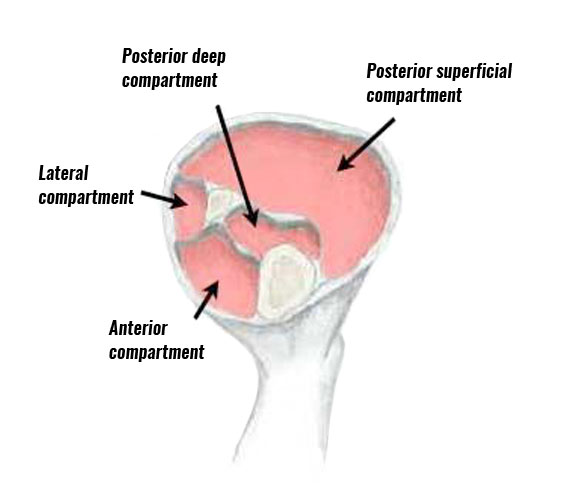
The posterior deep compartment of the lower leg is surrounded by a sheath and contains the flexor hallucis longus, the flexor digitorum longus and tibialis posterior muscles.
Occasionally in some people, an additional sheath surrounds the tibialis posterior muscle.
Acute compartment syndrome
Acute compartment syndrome is caused by impact or trauma which causes bleeding within the muscle compartment. The swelling increases pressure inside the compartment resulting in pain. A muscle strain can also bleed within a muscle compartment having the same effect.
Chronic compartment syndrome
Chronic compartment syndrome usually comes on over a longer period of time through overuse. The muscle grows too big for the compartment or sheath that surrounds it increasing pressure within the compartment and causing pain. Biomechanical factors, such as overpronation where the foot rolls in or flattens too much when running can abnormally increase the load on certain muscles making compartment syndrome more likely.
Treatment for posterior compartment syndrome
Acute injuries
Immediate medical attention should be sought for severe acute compartment syndrome as long-term damage to nerves and muscles can occur.
A doctor may prescribe anti-inflammatory medication e.g. Ibuprofen to help reduce pain and swelling and in more severe cases surgery may be indicated.
Always check with a doctor before taking medication.
Chronic compartment syndromes
Treatment for chronic compartment syndrome is rest. Simply reducing running mileage, or training load to 50% of normal may be enough.
However, switching to other forms of exercise such as cycling or swimming, or even complete rest may be needed.
Apply ice or cold therapy for up to 20 minutes at a time. Use a wet tea towel or commercially available cold packs to avoid skin burns.

Massage
Soft tissue massage and myofascial techniques may help relieve muscle tightness and improve comfort in some patients. However, there is limited evidence that massage alone can resolve chronic exertional compartment syndrome.
Gait analysis
Full gait analysis can be done to analyze running style and any biomechanical dysfunction of the foot, especially overpronation where the foot rolls in or flattens.
This causes the muscles of the lower leg to work harder than they might otherwise, leading to muscle growth (hypertrophy) and therefore a chronic compartment syndrome.
Overpronation can be corrected with orthotic inserts which are placed into the shoes to correct the motion of the foot, which in turn will reduce the load on certain muscles in the lower leg.
Surgery for posterior compartment syndrome
If symptoms do not improve with rest and activity modification, surgery may be recommended.
The operation, known as a fasciotomy, involves making one or more small incisions in the lower leg and cutting the fascia (the sheath surrounding the muscle compartment). This releases pressure within the compartment and allows the muscles to expand more normally during exercise.
If more than one compartment is affected, multiple compartments may be released during the same operation. Most athletes can gradually return to training once the wounds have healed and strength has returned. As with any operation, there are risks including infection, nerve injury, scarring and persistent symptoms.
Recovery time
Acute compartment syndrome: Following emergency surgery, recovery may take several months depending on the severity of muscle and nerve damage.
Chronic exertional compartment syndrome: Mild cases may improve within a few weeks by reducing training load and correcting biomechanical factors. However, symptoms often return when activity levels increase. Athletes undergoing surgery typically return to sport within 6 to 12 weeks, although full recovery may take longer.
References
- Hislop M, Tierney P, Murray P et al. Chronic exertional compartment syndrome: the controversial “fifth” compartment of the leg. Am J Sports Med 2003;31(5):770-6
- Hutchinson M R, Bederka B, Kopplin M. Anatomic structures at risk during the minimal incision endoscopically assisted fascial compartment releases in the leg. Am J Sports Med 2003;31(5):764-9