Lisfranc injury is a dislocation or fracture in the midfoot area. It is very rare, however, vital that it is not missed because long-term damage can occur.
Medically reviewed by Dr Chaminda Goonetilleke, 20th Jan. 2022
Lisfranc injury symptoms
Symptoms of a Lisfranc fracture/dislocation include:
- Pain in the midfoot area.
- Swelling on the top of the foot.
- Difficulty putting weight on the foot.
- Sometimes bone deformity, but not always.
- Tenderness over the Lisfranc joint area.
- Increasing pain when pushing up onto your toes or performing a calf raise exercise.
Have I got a Lisfranc’s injury?
If your physio or doctor suspects a Lisfranc fracture/dislocation injury will X-ray the foot in a weight-bearing position. However, even with an X-ray, Lisfranc injuries are often missed. Therefore, if it is suspected, and not obvious on the X-ray then an MRI or bone scan confirms the diagnosis.


What is a Lisfranc injury?
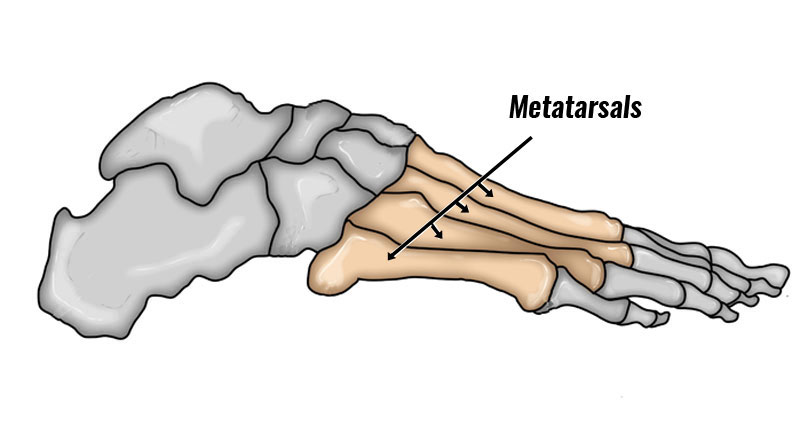
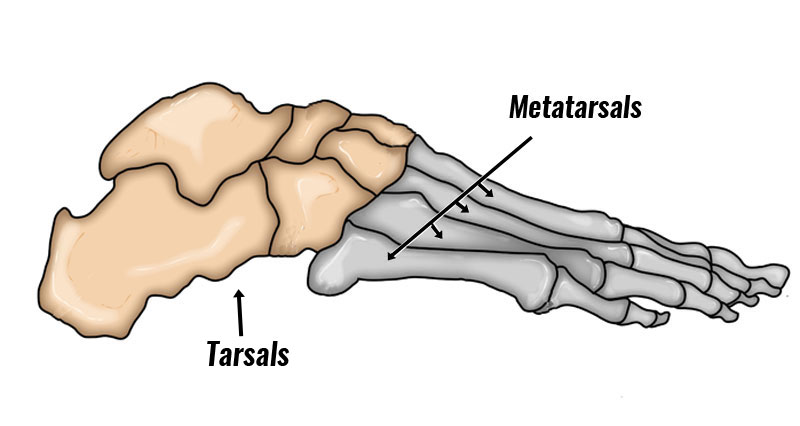
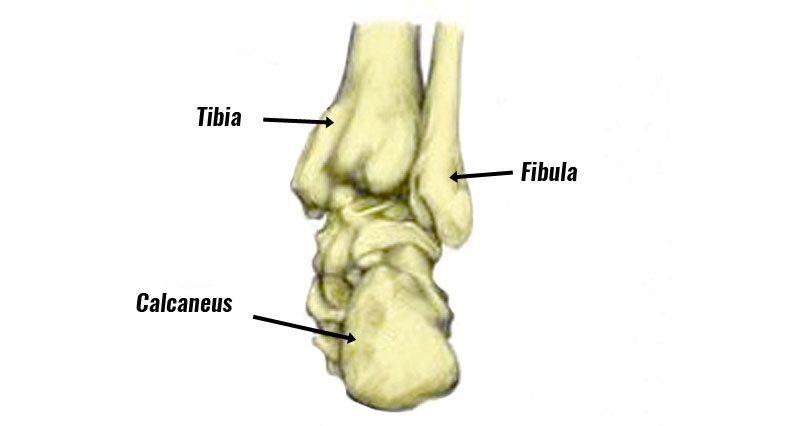
The term Lisfranc joint refers to the tarsometatarsal joints where the short tarsal bones in the midfoot meet the long bones or metatarsals in the foot. Jaques Lisfranc was a surgeon in Napoleon’s army who described an operation for amputation through this joint.
Lisfranc injury, or Lisfranc fracture-dislocation, is rare in sport but if left untreated it can have very severe consequences. If you suspect a midfoot sprain then you should always consider it a possibility.

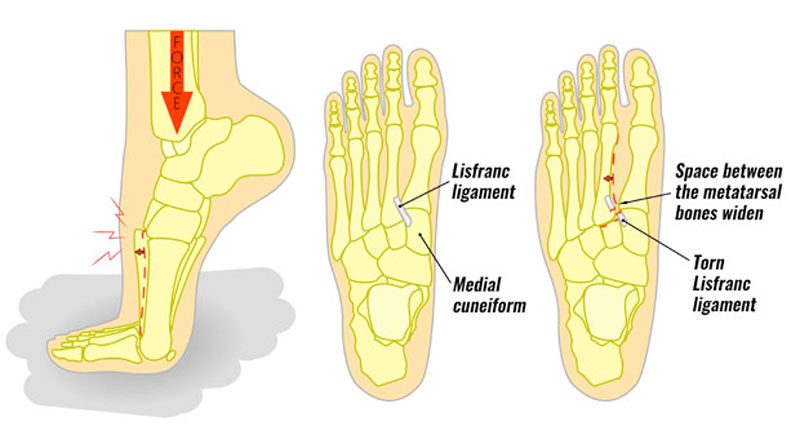
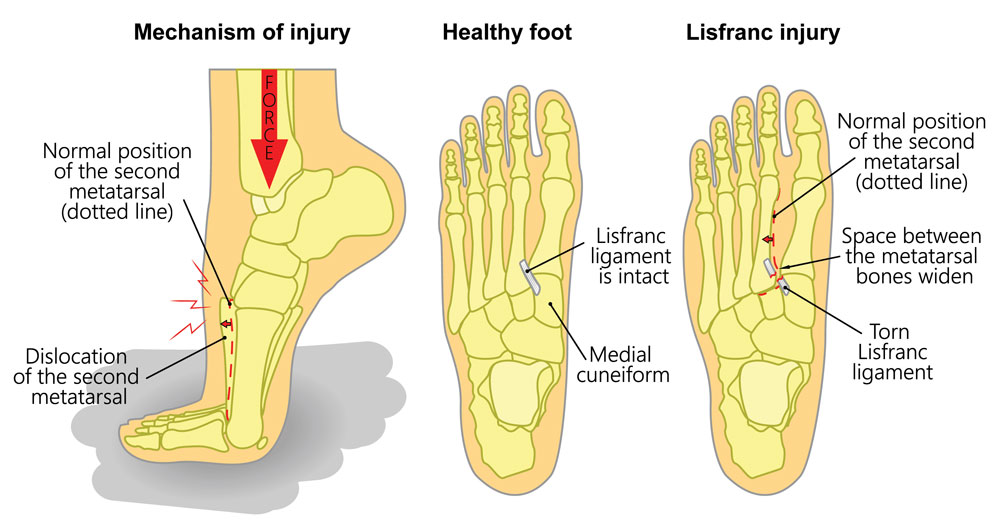
The most common cause is stepping into a small hole, which causes a strong twisting force with a lot of body weight on top. It also occurs in road traffic accidents.
The lisfranc ligament connects the medial cuneiform bone (one of the tarsals) to the base of the 2nd metatarsal. The injury may consist of a dislocation where there is only ligament damage or a fracture of one of the two bones may also occur.
Treatment
If you suspect this or even a midtarsal joint sprain, then seek medical advice immediately. Delaying treatment of Lisfranc injury can cause long-term or permanent damage.

If confirmed, a plaster cast with a toe plate extending under the toes is applied below the knee to immobilize the joint. Sometimes the bones require fixing with pins or wires.
Treatment will then depend on the severity of the injury. Precise anatomic reduction of the bones is required. If this is the case then the cast is usually on for 4 to 6 weeks.
After this time foot and lower leg rehabilitation exercises restore mobility, strength, and proprioception.