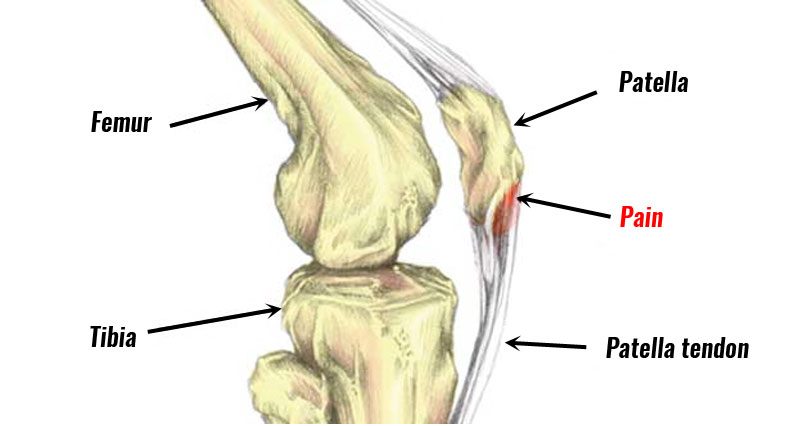
Patellar tendonitis (also known as patellar tendinopathy or Jumper’s knee) is an overuse injury that causes pain at the front of the knee, specifically at the bottom of the patella (kneecap). Here, we explain the symptoms, causes, and treatment of Jumper’s knee. We also provide a step-by-step rehabilitation program to guide you from injury to full recovery.
Patellar tendonitis symptoms
Symptoms usually develop gradually over time and include:
- Pain at the bottom of the patella (kneecap), known as the lower pole of the patella
- Contracting your quadriceps muscles or squatting is painful
- Aching and stiffness after exercise
- At times chronic pain may flare up and be acutely painful
- Pressing in over the bottom of the patella will be tender
- Thickening of the affected tendon
- In particular, jumping activities cause most pain or discomfort, hence the term Jumper’s knee.
How bad is my Jumper’s Knee?
Jumper’s knee injuries are graded from 1 to 4 depending on how bad your pain is.
Grade:
- 1: Pain only after training.
- 2: Pain before and after training but the pain eases once warmed up.
- 3: Pain during training which limits your performance
- 4: Pain during everyday activities
Other signs include a weak or atrophied vastus medialis oblique (VMO) muscle on the inside of the thigh, as well as weakness in the calf muscles.

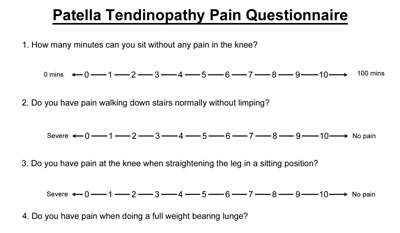
VISA pain questionnaire for Patellar tendonitis
The VISA pain questionnaire is excellent for monitoring symptoms which can often be difficult to describe or measure with a long-term chronic condition. The lower your score, the worse your injury. Do this regularly, for example, once per week to measure progress.
Download Jumper’s Knee pain questionnaire
Warning!! – This injury may seem like a niggling injury that is not that bad. Many athletes continue to train and compete on it as it may not be a debilitating injury and recovers after a short period of rest. However, neglect jumper’s knee at your peril. If left to become chronic, it can be very difficult to treat and may require surgery.
View injuries with symptoms: Aching knee / Knee pain kneeling / Pain below the knee

What is Patellar tendonitis?
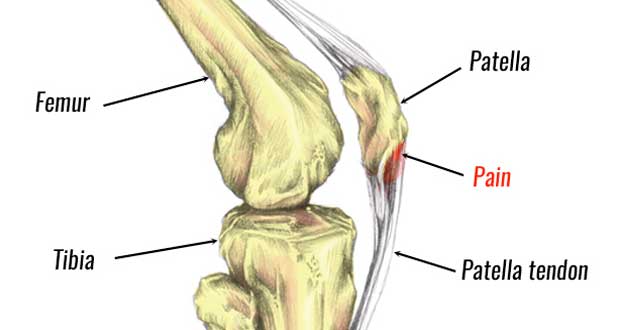
Patella tendonitis is inflammation of the patella tendon at the front of the knee. In chronic, long-term cases, wear and tear or degeneration is more likely than acute inflammation, hence the term ‘ Patella tendinopathy‘ is often more appropriate. For the purposes of this article, we interchange the terms Patella tendonitis and tendinopathy.
The patella tendon, also known as the patella ligament, is extremely strong. It joins the patella (kneecap), to the shin bone or tibia. The large quadriceps muscles at the front of the thigh pull on the kneecap, producing huge forces through the patella tendon, especially when jumping and landing.
What causes Jumper’s knee/Patella tendonitis?
Jumper’s knee is an overuse injury. In practice, the majority of chronic cases are more likely to be degeneration of the tendon rather than acute inflammation, which should settle down after a few days’ rest.
With repeated strain, micro-tears and collagen degeneration occur in the tendon. This is known as patellar tendinopathy or Jumper’s Knee.
Although it is an overuse injury there are a number of factors that make people more likely to suffer including poor foot biomechanics, weak quadriceps muscles, and incorrect training practices.
Q angle of the knee & VMO
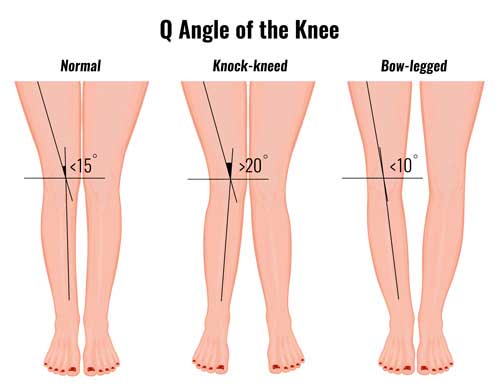
The Q angle of the knee refers to the angle of the femur (thigh bone) to the tibia (shin bone). Often athletes with patella tendonitis also have weak Vastus medialis oblique (VMO) muscles. This is the muscle on the inside of the quadriceps near the knee. Additionally, they may also have significant calf muscle weakness.
Patellar tendonitis treatment
The aims of treatment for Patellar tendonitis are to reduce pain, stretch the quadriceps muscles in particular, then gradually increase the load through your patella tendon.
- To reduce pain
- Stretch the quadriceps muscles
- Gradually increase the load through your knee
Cold therapy
Apply the PRICE principles of protection, rest, ice compression, and elevation. Apply cold or ice for 10 minutes every couple of hours, especially during the first 24 to 48 hours as well as after exercise. Reduce frequency as your symptoms improve.
Jumpers knee taping

A simple patella tendon taping technique helps relieve the symptoms of patella tendonitis. Applying tape around the bottom of the knee compresses the tendon. As a result, the direction of forces transmitted through the tendon change. Therefore relieving pain.

Patella tendonitis strap

Wear a knee support, or jumper’s knee strap to reduce pain and ease the strain on the tendon. This works the same as taping but is more convenient for most.
Medication
A doctor may prescribe anti-inflammatory medication e.g. ibuprofen. It is thought that anti-inflammatory medication may help in the short term with acute inflammation and pain but may even hinder healing later on. Do not take ibuprofen if you have asthma and check with a doctor before taking any medication.
Electrotherapy
A professional therapist may use electrotherapy in the form of ultrasound or laser treatment to reduce pain and inflammation and aid the healing process
Massage

Cross-friction massage for Patella tendonitis involves applying deep pressure transversely across the tendon. It is often used for more chronic cases as the frictions help realign new fibres. Also, deep friction massage may trigger an acute response, stimulating the healing process. Thigh massage may help loosen thigh muscles and increase the effectiveness of stretching exercises.
Injections
Aprotinin injections may help tendinopathies by restoring enzyme balance in the tendon. If the knee does not respond to conservative treatment, surgery may be required.
Exercises for Patella tendonitis
The following exercises form part of our comprehensive Patella tendonitis rehabilitation program. In the early stages quadriceps stretching is most important. Later, progressively more difficult strengthening exercises gradually increase the load through your tendon.
Quadriceps stretch

Stretch the quadriceps muscles regularly throughout the day. This lengthens the muscles, therefore placing less stress on the tendon. Keep your knees together and gently pull your leg up. You should feel a stretch at the front of the leg which should not be painful. Hold the stretch for 30 seconds and repeat with a short break in between. Aim to do this exercise 1-2 times per day minimuim.
Strengthening

Strengthening begins with isometric or static exercises. If you have access to a leg press machine at a gym then this is perfect, but not essential. Then, slow, heavier lifts before progressing onto eccentric leg exercises. Eccentric strengthening exercises are the most important and thought to stimulate healing in cases of Patellar tendonitis. These involve the quadriceps muscles lengthening whilst also contracting.
Other exercises
Our full rehab program includes exercises, movement control and function exercises. Activation exercises to keep the hip and gluteal muscles firing Movement control or proprioception exercises improve your coordination, balance and spatial awareness. Functional exercises are more dynamic and sports-specific and include agility drills and exercises.
- View more exercises for Patellar tendonitis
Surgery for Patellar tendonitis
The surgical procedure for treating jumpers knee varies depending on the individual and the surgeon’s preference. Success rates are aroung 60-80% and it could take 6 to 12 months to return to competition after surgery. Surgery may be indicated only after conservative methods have been properly tried first.
Similar injuries
The following injuries have symptoms similar to Patella tendonitis:
- Patella tendon rupture is a tear of the patella tendon and can be either complete or partial. It is often caused by an explosive jumping or landing action and may follow a chronic case of patella tendonitis.
- Osgood Schlatter disease is a common cause of knee pain in children and causes pain at the front and just below the knee.
- Sinding-Larsen-Johansson Lesion or syndrome causes symptoms very similar to Jumper’s knee, but occurs in young athletes and children and is more like Osgood-Schlatter disease.
References & research
- Blazina ME, Kerlan RK, Jobe FW et al. Jumper’s knee. Orthop Clin Nirth Am 1973;4(3):665-78
- Kahn KM, Bonar F, Desmon PM et al. Patella tendinosis (jumper’s knee): findings at histopathologic examination, US and MR imaging. Radiology 1996;200(3):821-7
- Maffuli N, Khan KM, Puddu G. Overuse tendon conditions. Time to change a confusing terminology. Arthroscopy 1998;14:840-3
Jumper’s Knee Pain Assessment
Move the sliders to match your pain or activity level.


