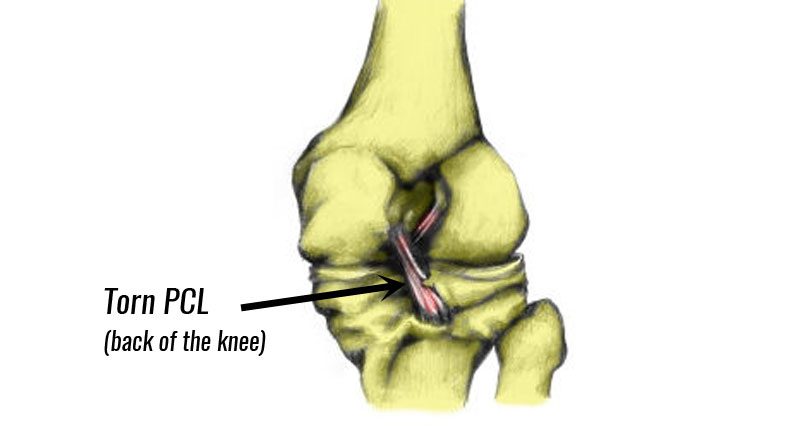
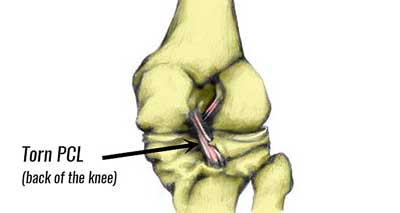
A torn PCL is a rupture (sprain) of the posterior cruciate ligament in the knee joint. One cause is an impact to the front of the knee which causes your knee joint to bend back the wrong way.
Medically reviewed by Dr Chaminda Goonetilleke, 2nd Jan 2022
PCL injury symptoms
Symptoms of a PCL injury typically include:
- Sudden onset, acute knee pain at the time of injury.
- Over time, you may also feel pain radiating into the back of the lower leg.
- You may have swelling in the knee joint, although this may be minimal.
- Your knee may also feel unstable, as if it is likely to give way, especially walking downstairs.
Diagnosis & assessment
If your knee is very painful and swollen it is unlikely that a full examination is possible. Once pain and swelling have subsided your physio can examine the knee more easily.
A professional therapist may do a number of knee assessment tests to help diagnose a posterior cruciate ligament injury. In particular, the posterior draw test and the reverse Lachman’s test.
Posterior drawer test
The posterior drawer test involves pushing the Tibia (shin bone)
Posterior sag test
The posterior sag test assesses laxity in the PCL. If the Tibia drops down, forming a sag or dent at the front of the upper shin then the test is positive. Always compare one knee to the other.
Skyline test
The skyline test assesses the level of displacement or sag when the tibia is held horizontally to the floor.
How bad is my PCL injury?
We grade PCL tears 1 to 3 depending on severity. Level 3 is the most severe. More severe injuries have greater backward tibial displacement. This is because the PCL is partially or completely torn.
In extreme cases, the ligament may become avulsed or pulled off the bone completely.

Imaging
Your doctor or physio may use an MRI scan and/or X-ray to assess the extent of the damage.
What causes a PCL injury?
The incidence of PCL injuries is less than that of the anterior cruciate ligament. This is mainly due to the greater thickness and strength of the ligament. Nevertheless, the most common way in which the PCL is injured is by direct impact to the front of the tibia itself, usually when the knee is bent.
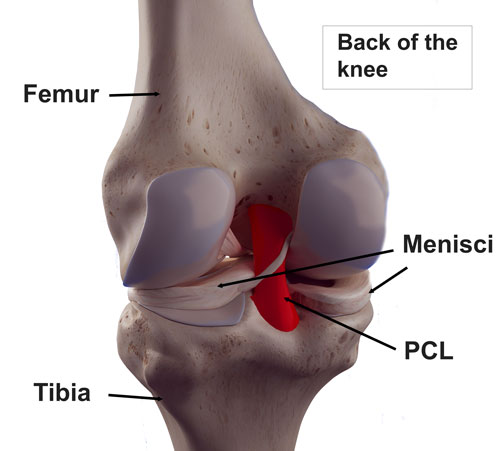
This may occur in a front-on tackle or collision or when falling with the knee bent. The injury is commonly associated with injuries to other structures in the rear compartment of the knee joint such as lateral meniscus tears. In addition, the articular cartilage may also be damaged.
Treatment for posterior cruciate ligament sprain
Immediate first aid is to apply the principles of PRICE (protection, rest, ice, compression, and elevation). Once you have an accurate diagnosis, two modes of treatment are available. These are conservative treatments or surgery.
Cold therapy
Apply a cold therapy and compression wrap as soon as possible after injury for 10 to 15 minutes every hour. Reduce frequency as your symptoms improve. This initial acute phase lasts 24 to 48 hours, or longer for more severe injuries.
Do not apply ice directly to the skin as it may cause ice burns. Wrap in a wet tea towel. Or, better still use a commercially available cold compression wrap.
Knee supports
Wear knee support or brace to protect the joint, especially in the early to mid-stage. A hinged knee brace provides the most support.
Specialist hinged knee braces that restrict the amount of flexion in the knee are the best type of brace. This is because they protect the PCL and help prevent over-straightening the knee.
Taping
The aim of PCL taping is to provide support for the ligament and prevent the knee from hyperextending (bending the wrong way) during healing or to give support and confidence during rehabilitation.
Exercises
A full rehabilitation program is important. This consists of mobility, stretching, strengthening, movement control, activation, functional, and sports-specific exercises.

Surgery for PCL injury
Expert interview: Mr Richard Villar, leading Orthopaedic Surgeon and former Surgeon to the British Army Special Air Service Regiment, explains posterior cruciate ligament surgery.
A lesser proportion of PCL injuries require surgical intervention. However, in more serious cases, in particular, in those in which other structures within the knee joint have been injured, surgery may be recommended. Surgery may also be indicated if the conservative management has not aided the stability of the knee sufficiently over a period of time.
In general, those who have sustained a PCL injury normally have good recovery rates, with most being able to return to sporting activities at the same level as before the injury. However, full recovery from cruciate ligament damage is highly dependent on the ability to adhere to a strict rehabilitation program.

The posterior cruciate ligament is torn less frequently than an ACL injury although it is much more demanding to deal with surgically. Usually, the first step with a PCL rupture is to try conservative treatment, such as physiotherapy and strengthening exercises. If this is unsuccessful, bracing may be attempted before surgery is undertaken. The procedure for a PCL reconstruction is similar to the ACL operation whereby it is an intra-articular operation using a bone-tendon-bone graft to create a new ligament.
Recovery from PCL reconstruction surgery is initially quite quick from the surgery itself to getting back on your feet, although it is a long process to get back to sports. Villar recommends a minimum of 6 months and up to a year.

