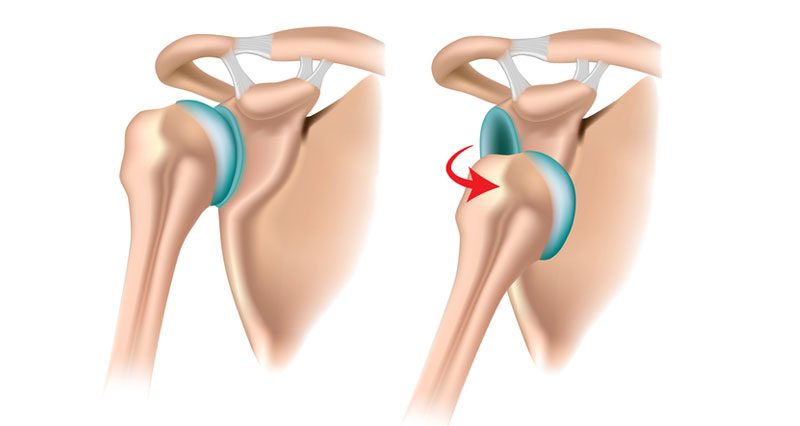
A dislocated shoulder occurs when the humerus bone displaces out of the joint. An anterior dislocation is most common where the humerus dislaces forwards out of the front of the joint. If you suspect a dislocated shoulder, seek immediate medical attention. Do not attempt to put the joint back into place.
Dislocated shoulder symptoms
Symptoms of a shoulder dislocation include:
- Sudden severe pain at the time of injury
- Rapid shoulder joint swelling
- Bruising usually develops later
- Feeling your shoulder has popped out of the joint
Also, the injured side often looks different or possibly lower than the uninjured side. The patient may hold their arm close to their body are often in severe pain. If nerve or blood vessel damage occurs, they may also feel pins and needles, numbness or discolouration through the arm to the hand.
What is a shoulder dislocation?
A dislocated shoulder occurs when the head of the humerus (upper arm) bone pops out of the shoulder joint. They are usually either posterior or anterior dislocations.
Anterior shoulder dislocations
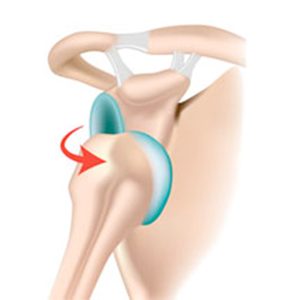
Most dislocated shoulders are anterior dislocations. Specifically, they occur in approximately 95% of injuries. The head of the humerus bone dislocates forwards, out the front of the joint. This happens when the arm is out to the side (abducted) and rotated outwards (externally rotated).
Posterior shoulder dislocations
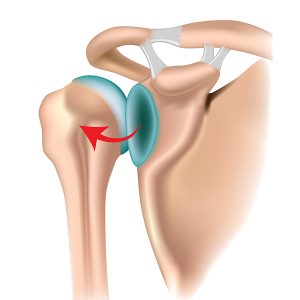
Posterior dislocations occur when the head of the humerus dislocates out of the back of the joint and account for around 3% of shoulder dislocations. They occur during epileptic seizures, or from falling onto an outstretched hand.
Read more on Posterior shoulder dislocation.
Anatomy
If you have dislocated your shoulder then you are likely to have damage to the surrounding ligaments, tendons, nerves, and blood vessels and possibly even fractures.
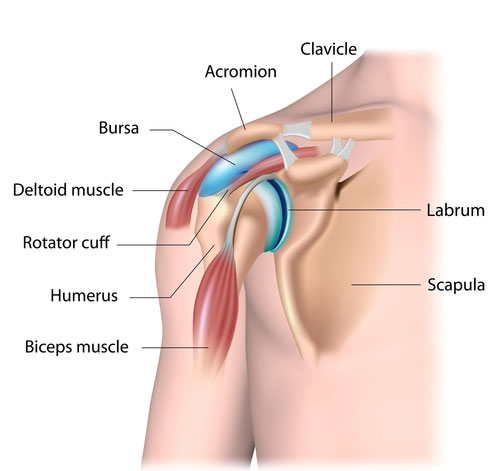
Most shoulder dislocations also result in glenoid labrum tears (Bankart lesions). The glenoid labrum is a ring of cartilage which acts like a cup, in which the humerus bone rests. In addition, Axillary nerve injuries also occur with dislocated shoulders. As a result, the patient has altered sensation or numbness over the outside of the shoulder. Recurring injuries are common. Therefore, shoulder rehabilitation is especially important.
Dislocated shoulder causes
Dislocated shoulders result from falling onto an outstretched arm, twisting your arm, or from direct impact on the shoulder. The shoulder joint is particularly prone to injury because it has a large range of movement. However, the increased range of movement sacrifices joint stability. Therefore making the shoulder more susceptible to injury.
Treatment
Immediate treatment for a dislocated shoulder has two stages. First, protect your shoulder joint preventing further damage. Secondly, seek medical attention as soon as possible. Never attempt to pop the shoulder back in yourself. This is because you may cause serious damage to nerves and other blood vessels if not done correctly.
Immediate First Aid
Stop playing immediately and seek emergency medical attention. It is likely you will not have a choice about this, as a dislocated shoulder is very painful. A doctor confirms your dislocated shoulder and carries out a reduction (puts it back into place).
Cold therapy/ice
Apply ice or cold therapy for 15 minutes every hour to help with the pain and swelling. Specialist cold therapy shoulder wraps are particularly good as they apply both cold therapy and compression at the same time.
Protection
If a Doctor cannot perform a reduction immediately, they may use a sling to take the weight off your arm. Later, after the initial acute period, a shoulder brace/support helps to restrict unwanted joint movement.
Dislocated shoulder reduction
Reduction is the medical term used to describe relocating a dislocated bone back into the right position. The sooner your doctor reduces your shoulder the easier it will be to reduce it.
A closed reduction is without surgery, whilst an open reduction involves an operation. The decision of whether to surgically reduce your shoulder may depend on any associated injuries, fractures and damage to your joint. An X-Ray follows reduction to check for possible complications.
Your doctor may give you an injection of 10-15ml of xylocaine to reduce pain, and muscle spasms and therefore aid reduction.
Surgery
Your surgeon usually operates as soon as possible after your injury. However, the decision over which approach to use depends largely on your lifestyle and activity.
Patients aged 15 to 25
Evidence suggests that young, active adults between the ages of 15 and 25 benefit from surgical reduction for a first-time anterior dislocation. The recurrence rate and quality of life outcomes appear to be better than for nonsurgical reduction.
Patients aged 25 to 40
Patients aged 25 to 40 are often encouraged to try conservative treatment first, because the recurrence rate is lower in older patients. Some surgical procedures result in reduced shoulder external rotation. Therefore they are not suitable for throwing or racket sports because of the effect on performance.
Recurrent shoulder dislocations
Unfortunately, recurrent dislocations are frequent, especially in younger athletes. Often arthroscopic surgery is done to investigate the damage done and/or stabilize your joint. The chance of suffering another dislocated shoulder is reduced to less than 5% following surgical repair.
Treatment after reduction
Treatment following a closed reduction is often referred to as conservative treatment. It means non-surgical and usually involves a period of rest and immobilization in a sling or similar.
This is to allow the structures which may have been injured to have adequate time to heal. Some surgeons advocate immobilizing your shoulder in 30 degrees of external rotation. This is because using a traditional sling in internal rotation (across your front), can make a Bankart lesion worse.
Although it may be very inconvenient, immobilising at 30 degrees may reduce the chance of your injury recurring. You may be prescribed NSAIDs such as ibuprofen to ease pain and inflammation.
Dislocated shoulder rehabilitation
Your shoulder will need extensive rehabilitation to regain mobility and strength. Following a reduction, you will usually be advised to rest and immobilize your shoulder in a sling for 5-7 days, longer if there are fractures or severe soft tissue damage.
After the period of initial immobilization, exercises to gradually increase your range of pain-free movement are done. Eventually, isometric strengthening exercises, dynamic strengthening, proprioception and functional or sports-related should be done.
References
- Smits-Engelsman B, Klerks M, Kirby A. Beighton score: a valid measure for generalized hypermobility in children. J Pediatr 2011;158(1):119–23, 123.e1–4.
- Gagey OJ, Gagey N. The hyperabduction test. J Bone Joint Surg Br 2001;83(1):69–74.

